Introduction
To see the whole slide imaging (WSI), please register to pathpresenter for once.
There is no charge for this registration.
History
61 yo, M
Trismus, pain and swelling
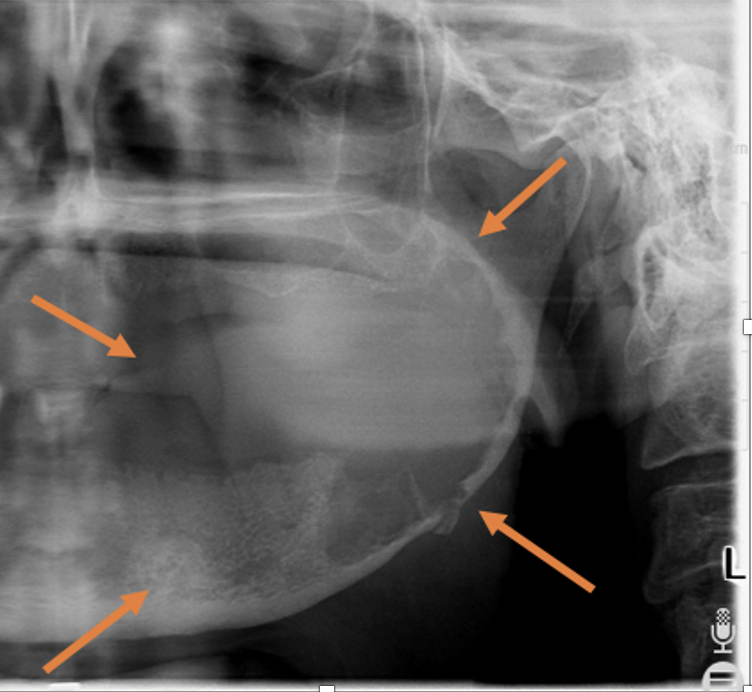
Large radiolucent lesion of the posterior mandible with soft tissue extension
Gross Findings
Incisional biopsy was performed only from the soft tissue extension due to trismus. Whole tissues measuring 1.5×1.5×1 cm were entirely submitted.
Microscopic Findings
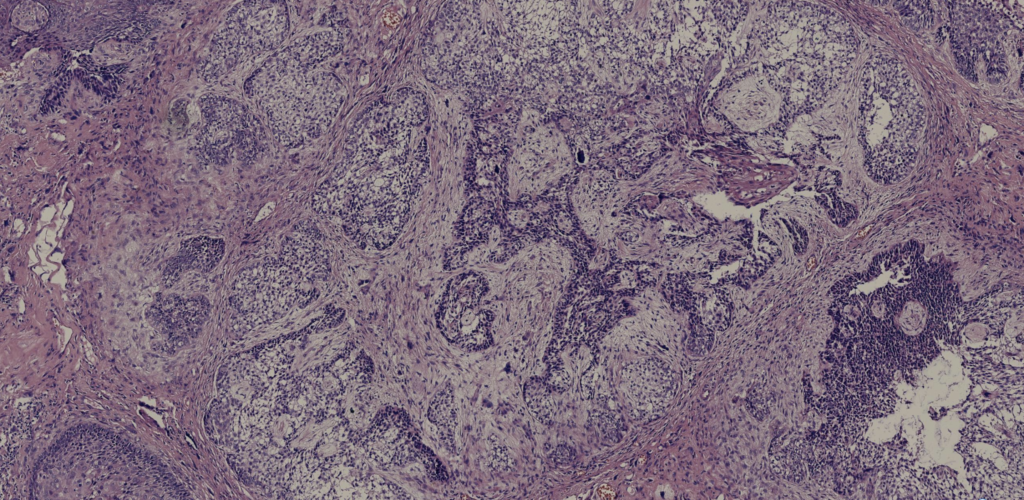
Final Diagnosis:
AMELOBLASTIC CARCINOMA
- Accounts for ≤2% of all odontogenic tumors
- 30% of malignant odontogenic tumors
- A wide age range is affected with a median age of 49 years
- Male predilection
- Mandibular predilection, usually posteriorly
- Jaw or orofacial swelling, sometimes with pain and paraesthesia common symptoms
Treatment
- The main treatment is radical surgical resection
- RT for non-surgical candidates
- Lung metastasis develops much more commonly than locoregional lymph node metastasis
- The 5-year overall survival rate is 70%, better after complete surgical resection
- Novel treatment considerations include proton beam therapy and BRAF targeted agents
Take-Home Messages
- Benign ameloblastoma may be present as a precursor lesion
- Differential diagnosis includes;
- Benign ameloblastoma, especially maxillary examples that can show high cellularity.
- Basaloid AC must be separated from basal cell ameloblastoma, basaloid squamous cell carcinoma and adamantinoma-like Ewing tumour
- With spindle cell changes warrants exclusion of spindle cell/sarcomatoid squamous cell carcinoma , carcinosarcoma and other spindle cell malignancies
- A primary intraosseous carcinoma lacking ameloblastoma features may be better categorised as primary intraosseous carcinoma.
